XVI - Contractual Arrangements for Programme Implementation
XVI.0 - Introduction to Contractual Arrangements for Programme Implementation
During the Country Cooperation Strategy (CCS), Country Support Plan (CSP) and Programme Budget (PB) formulation, country offices determine with the government how to establish appropriate mechanisms for the implementation of the country programme. Similarly, HQ Budget Centres formulate their workplans to execute the Programme Budget. This requires careful consideration of the implementation modality to be used, meaning the management and delivery of programme activities and resources to achieve specified results as set forth in the work plans. This includes identifying if work should be undertaken internally by WHO staff or with whom WHO must work to best achieve the results, including government agencies, such as the Ministry of Health, departments, agencies, institutions, etc.; non-profit organizations, e.g., international, national, provincial, or local Non-governmental Organizations (NGOs) or Community Service Organizations (CSOs); research and academic institutions; or other United Nations entities; as well as how to engage with them.
The following implementation modalities are available:
- National implementation: when the government (i.e. Ministry of Health), a department within the ministry, or a wholly owned government entity (university, a regional or local authority or a municipality) implements one or more of the outputs in the programme. This includes:
- When the WHO country office provides the funds to the government entity for their implementation (Direct Financial Cooperation or DFC); or
- When the WHO country office makes payments to personnel hired (or designated) by the government to implement activities where the government is not able to or the risk is assessed as high for the government to make the payment directly (Direct Implementation or DI). In this case, the WHO pays the end recipients directly and no funds are transferred to the government.
2. WHO implementation: WHO must have the technical and administrative capacity to assume the responsibility for mobilizing and applying effectively the required inputs to reach the expected outputs, and following policies and procedures established for its own operations.
a. Internal implementation can be completed by either:
- utilizing WHO personnel or consultants (where the planning and assignment of work to be undertaken falls under human resources – eManual section III); or
- procuring goods and services – using a commercial contract where WHO receives goods or services in return for a defined contract. Procurement should be undertkane as part of the procurement plan to purchase goods and services (agreement for performance of work, non-grant letters of agreement etc.) and falls under procurement (eManual section VI)
- Issue grants to non-governmental organizations/non-state actors to support the grant recipient's work or implement activities to achieve a WHO programmatic result, using a Grant Letter of Agreement (GLOA);
- Enter into Technical Services Agreements for research or other technical projects/investigations.
3. United Nations agency implementation, either by using them directly as an implementing partner (using GLOA), establishing a joint programme or having them undertake activities in a WHO-implemented activity (service procurement).
These implementing modalities are not mutually exclusive and can be used collectively to achieve WHO workplan results. Furthermore, WHO may support national implementation by undertaking activities, for example, procurement or recruitment activities (especially where the capacity assessment highlights weaknesses in these areas), or activities such as organizing strategic events or conferences, and producing outputs such as research products.
It is the responsibility of the WHO Country Office and HQ Departments to select the most appropriate implementation modality. In doing so they must also determine whether WHO will implement the activities, or if the activities will be entrusted to an implementing partner, and to identify the partners required to achieve the programme outputs considering their capacity and related risks. Partners include government agencies, such as ministries, departments, agencies, institutions, etc.; non-profit organizations, e.g., international, national, provincial or local NGOs or CSOs, as well as research and academic institutions; or another United Nations entity.
The implementing partner (IP) is the entity which assumes full responsibility and accountability for the effective use of WHO resources, the implementation of activities as defined in the mutually agreed workplan, and the achievement of outputs. An implementing partner must have sufficient programmatic, managerial, technical, financial, and procurement capacity to both implement WHO resources, and monitor progress of the implementation.
If another UN entity is selected, in a country context the UNCT should be able to identify specific members able to work on different results based on their mandates, capacity and available resources. Where joint programming is undertaken, WHO should work with its partner UN agencies to ensure that cash transfer modalities are aligned, noting that the risk tolerances may be different for the other agencies, depending on the size of the partner and the activity, however a common approach should be undertaken with a joint programme with common IPs.
This selection must be based on a risk assessment and the capacity of both the implementing partner and the country office or department. Implementation modalities at the country level must be discussed and agreed upon with the MOH.
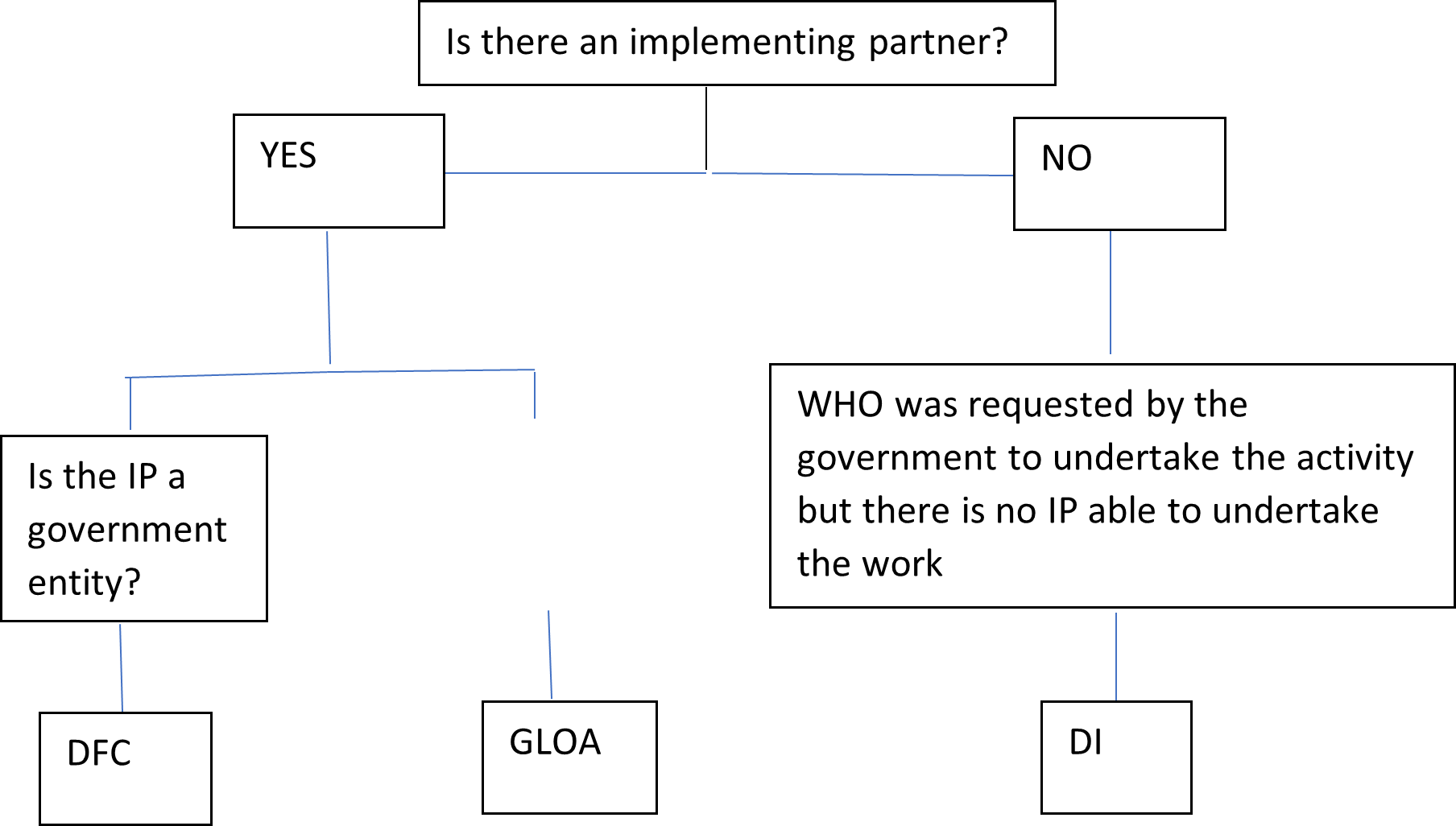
Activities may be undertaken through different implementation and contractual modalities depending on the optimal means of undertaking the activity. For example, where an immunization campaign is undertaken by a government, with funding from WHO, the activity would fall under DFC. Funding for an immunization campaign could also be granted and undertaken by an NGO – in this case a GLOA would be used. In certain situations, there is no government entity or NGO that can undertake the work and instead WHO directly oversees the immunization campaign – in this case payments to vaccinators contracted by the government but overseen by WHO is treated as Direct Implementation. For DI, please refer to eManual section XVI.4.
An Implementing Partner (IP) includes government entities; and non-state actors (non-governmental organizations (NGO), not-for-profits, foundations etc.); and UN Agencies.
In summary:
To assist in distinguishing between when to use Direct Financial Cooperation and Grant Letter of Agreements please refer to the following table for guidance:
Comparison of DFC, GLOA and DI:
| | DFC | GLOA | DI |
| Purpose | To make payments to cover costs of items or activities that would otherwise be borne by governments, enhancing their health development capacity and meeting commitments under WHO's Programme Budget and technical cooperation at the country level. Components can include the following costs: - operational costs of public health activities, such as immunization campaigns
- national seminars or training courses
- field travel for WHO programmes
| To transfer funds to non-state actor Implementing Partners (IPs) to achieve a programmatic result under WHO's Programme Budget. This includes the following activities: To assist an IP reach specific goals in the IPs work (e.g. research projects) in line with WHO's own objectives To support WHO and national partners achieve health related objectives (including by providing support at country level to improve the health of the populations). To implement activities on behalf of WHO or government, but funded by WHO when DFC is not possible (e.g. grant to an NGO who is best placed to complete the activity where WHO or a government cannot). | Used when WHO makes payments directly to recipients for implementing activities, when standard contracts of DFC and GLOA are not possible |
Beneficiaries | Government agencies | Non-State Actors including: nongovernmental organizations, academic institutions, UN Organizations, Intergovernmental organizations (entities created by treaty, involving two or more nations). Excludes private sector entities and business associations. | Payments are made directly to end recipients without transferring funds to the Ministry of Health |
| Used by | Country office | Country office, regional offices and headquarter units | Country office |
| Legal requirements | The DFC contract generated through GSM requires WR/HCO signature and is then sent to the government for countersignature. The contract sets out the respective responsibilities of WHO and the implementing partner, including the expectations on the implementing partner for achieving results and sound financial management. The DFC contract is available on the LEG intranet: Library & Resources (sharepoint.com) | GLOAs are non-standard contracts and the terms and conditions are specific to the GLOA agreement. The standard template, prepared by LEG and FNM is available in the GLOA Standard Operating Procedures and the LEG intranet: Library & Resources (sharepoint.com). When working with UN Agencies, a standard agreement is also available on the LEG intranet. If the standard template is not used, the proposed agreement must be cleared by LEG before it can be finalized. | DI should only be initiated once it has been determined that other types of standard contracts (e.g. DFC, GLOA, APW, GES) are not possible. |
| Clearance of proposal | WHO standard delegation of authority | WHO standard delegation of authority and in addition: FENSA clearance Grant Review Committee clearance (for grants over $50,000) | WHO standard delegation of authority |
Purchase Orders | Service PO - DFC PO | Service PO - GLOA PO | Service PO – Imprest /Credit Card PO (IPO) |
| Payments | Full payments may be made upon signature of the DFC by both the contractual partner and WHO. When deemed necessary, payments may also be made in instalments and linked to deliverables in the signed agreement, which may include submission of interim technical reports and FACE reports to inform the release of subsequent tranches of funds. DFC payments are made in local currency. Cheques or bank transfers should, be made payable to a government, governmental agency or specific ministry, and not to individuals. | Payments are not issued in full upon the signing of the contract. Instead, a maximum of 50% of the total amount may be disbursed upfront at the time of signature. Additionally, at least 10% must be withheld until the final report has been received and formally accepted. When deemed necessary, payments may also be made in instalments and linked to deliverables in the signed agreement, which may include submission of interim technical reports and FACE reports to inform the release of subsequent tranches of funds. | For DI, the agreed payments are made to the final beneficiaries by: - Bank transfers from the Imprest bank account
- Payment services providers (banks, micro-finance institutions, money-transfer companies, post offices, mobile money payments providers etc.) that can be engaged to deliver and distribute cash payments based on WHO CO's authorization and instructions.
- Cash payments from the Imprest cash account: only in exceptional circumstances, when it has been established that no other payment modality can be used.
- Operational advances - refer to section XXXX
|
| Recording | The expenditure type for DFC activities is 511 – Direct Financial Cooperation. | The expenditure type for GLOA activities is 526 – Grant Letter of Agreement. | The expenditure type for DI activities is 527 – Direct Implementation. |
When selecting non-state actors as partners, it is important to assess where the appropriate instrument is a grant or a procurement action. The type of partner and responsibility for the programmatic output drives the decision on the appropriate contracting modality. The grants (GLOA) instrument is to be used contracting with non-state actors for the delivery of an output or for the financing of their activities, as aligned to WHO programme objectives, as an implementing partner (where it has full responsibility for an output) or a partner contributing to an output. A procurement contract is the appropriate instrument for purchasing inputs to a programmatic output, whether goods or services, which do not have the programmatic responsibility for the output and are typically (but not exclusively) provided by private sector entities.
Grant LOAs should be distinguished from Non-grant Letters of Agreement, which is the general term used to describe a contract with an external party which can be used for the procurement of services where it is not possible to use one of the standard service contracts (APW or Consultant Contract). Non-grant Letters of Agreement are described in more detail in eManual section VI.2.3.
To assist in distinguishing between the procurement of services (via a commercial contract) and a GLOA, please refer to the following table for guidance:
Comparison of procurement and GLOA
| Procurement | GLOA |
An exchange transaction is a mechanism for the procurement of a specific service or product with clear and specific obligations for both the buyer and the seller. An exchange transaction is one in which each party receives something and provides something of approximate equal value in return. | A non-exchange transaction is one in which one party receives something of value without directly returning value in exchange. An arrangement under which there is a transfer of funds, from WHO to a beneficiary: -To support the beneficiary reach specific goals in line with WHO's own objectives and priorities; -To support WHO in its mandate to support Member States in achieving global health related objectives (including by providing support at country level to improve the health of the local population). |
| Principal purpose and direct objectives are to acquire goods or services (either directly for WHO or for a Member State) | Principal purpose and direct objectives are to achieve public health related objectives. Funding assistance to achieve some result. |
| Product or service oriented | Purpose oriented |
| Normally an agreement with private sector entities but can be with UN agencies (e.g. contracting UNICEF to procure drugs) or other organizations | Generally provided to governments, academic institutions such as research institutes, NGOs, multigovernmental organizations |
| Payments are linked to the receipt of clear deliverables. | Payments are often made in advance or based on progress/ final reports and achievement of results. |
| If services or goods are not delivered, legal consequences exist. | Unspent balance, as well as incurred expenditure not in line with the agreed budget, needs to be refunded to WHO |
| Necessarily starts with a need expressed by WHO (either directly by or via a member state) | An application for funding can be received from the prospective grantee |
| Generally, no detailed line-wise budgets provided. | Implementation must be in line with the agreed budget with detailed lines by budget categories. |
| Ends with goods / services rendered being invoiced and these invoices paid. | Ends with technical and financial reports as evidence of the agreed activities having been conducted |

